 at the point of care")
Urinalysis laboratory diagnostics and its significance in addressing UTI
With around 400 million affected individuals globally, urinary tract infections (UTIs) are among the most frequent bacterial infections. UTIs lead to millions of medical consultations a year and put a significant strain on healthcare systems and societies [1,2], especially with UTIs and suspected UTIs accounting for 15 % of all antibiotics prescriptions in the US and Europe [2].
Despite their costly and time-consuming nature, urine cultures remain the gold standard in UTI diagnostics and account for up to 40% of the overall requested cultures in a lab. This workload can clog up resources in the laboratory. At the same time, clinicians frequently face an information gap where diagnostic information is not available, but treatment options are requested. Often, this results in the empiric prescription of antibiotics, even though up to 80% of suspected UTI cases turn out to be negative. Therefore, a fast and reliable method to exclude UTIs can be a driver for laboratory workflow improvements and antimicrobial stewardship, enhancing clinical decision support in the doctor’s office and in the hospital [3].
Improving UTI diagnostics
Rule out a UTI in less than a minute
With a diagnostic performance of 0.973 (AUC), the UF-series can provide quantitative information on bacteriuria in less than a minute. A recent investigation of different cut-off values revealed a bacteria count of ≥ 58 cells/μL as the most sensitive value for ruling out urinary tract infections with a sensitivity of 99.4 % (NPV 99.7 %) and a specificity of 78.2 % (PPV 65.4 %) [4].
Improving laboratory workloads
Considering the high rate of up to 80% of suspected UTI specimens that turn out to be negative, urinary flow cytometry and the direct exclusion of UTIs can support laboratory efficiency by reducing the amount of unnecessary urine cultures [2].
![[Sysmex MEA (english)] Infographic illustrating the gold standard of urine test strip analysis vs. urinary particle analysis and the features of each.](/fileadmin/_processed_/5/7/csm_Rule_out_UTI_in_less_than_a_minute_with_modern_diagnostics_7d8f38e0a5.jpg "SEU UTI Urin Web Illustration 2")
Supporting dAST
In a private laboratory setting, the combination of BACT (≥ 105/µL) and WBC (≥ 10/µL) counts allowed a direct rule-out of 42% of suspected UTI samples with direct reporting of negative results at the day of sample reception. In addition, it was shown that the ‘BACT Info’ flag (RUO) supports the assessment of the the gram status and may predict positive samples containing gram-negative bacteria, allowing direct antibiotic susceptibility testing (dAST). dAST can reduce response time for antibiotic profiles by up to 24 hours, and thus contribute to reduced empiric use of antibiotics and improved clinical decision making [5].
At the emergency department
In the context of an emergency department, the detection, classification and assessment of infectious conditions is of utmost importance. In a smart laboratory setup at the University Hospital San Juan de Alicante, UF-series and UC-series information is combined with individual patient data that allows the prediction of UTIs in the form of a UTI score. This score has been established for use by the San Juan de Alicante emergency department in a clinical routine, leading to improved prescription patterns for antibiotics and improved culture requesting with a positive impact on cost-effectiveness in this particular laboratory [Publication in preparation].
Fungal UTI
Since bacterial infections are not the only potential cause of a UTI, the YLC (yeast-like cell) parameter was demonstrated to support the exclusion of funguria with excellent diagnostic performance (NPV 100%) at a cut-off of 5 YLC/µL in comparison to Candida sp. culture, implying a positive impact on laboratory workflows and antimicrobial stewardship [6].
Distinguishing upper and lower UTI
In UTI-positive samples, the presence of renal tubular epithelial cells has been demonstrated to act as a supportive parameter to distinguish between an upper and lower urinary tract infection, thereby outperforming classical markers of an upper UTI [7].
AST in less than one hour in near-patient settings
In settings in which we do not have access to the microbiology laboratory, the PA-100 AST System offers the possibility of analysing native urine samples using a point of care tool. This automated analyser allows the detection of bacteriuria within 15 minutes and the performance of antibiotic susceptibility testing within 30 to 45 minutes. This opens the door to providing support for diagnoses that enable targeted antibiotic prescriptions within less than one hour, during the patient’s first visit to the doctor.
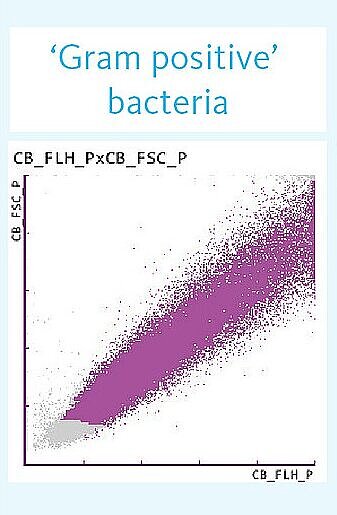
BACT info flag (RUO)
The BACT-info flag may provide additional information on the Gram dye affinity for samples positive for bacteriuria.
Suspicious samples are highlighted with any of the following flags:
Gram Positive?
Based on the distribution, it can be inferred that gram-positive bacteria are present.
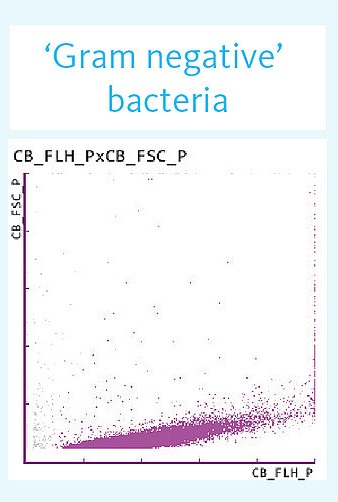
Gram Negative?
Based on the distribution, it can be inferred that gram-negative bacteria are present.
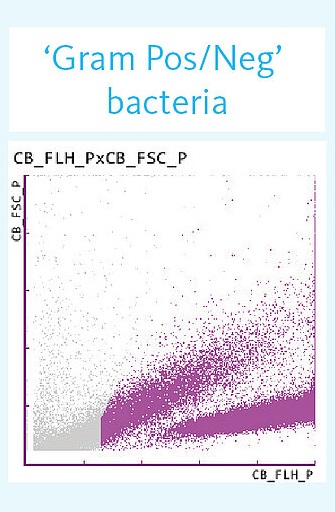
Gram Pos/Neg?
Based on the distribution, it can be inferred that gram-positive and gram-negative bacteria are present.
Unclassified
The class does not become clear from the distribution.
Gram-positive bacteria are detected with a sensitivity of 78% and a specificity of 96%, whereas for gram-negative bacteria, both the sensitivity and specificity reach 89%. This might allow an early initiation of antibiotic UTI therapy and more targeted follow-up diagnostics [DeRosa] or support the skip urine culture for gram-negative sample and proceed with a direct AST [Gilboe].
Antibiotic susceptibility testing (AST)
Fighting antimicrobial resistance
Due to a long diagnostic pathway and the prescription of empiric and unnecessary antibiotics, UTIs are already the fourth most common cause of AMR-related deaths [8]. For this and many other reasons, Sysmex is committed to better education and awareness regarding AMR around the globe. Learn more about the role of antibiotic susceptibility testing in fighting antimicrobial resistance worldwide and become a #AMRfighter by joining us in taking steps toward AMR mitigation and prevention.

References
[1] Foxman B (2014): Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden
[2] Keller, P. (2019): Ein neuer Schritt zur schnelleren Urinanalytik
[3] Kalsi, J., Arya, M., Wilson, P., & Mundy, A. (2003): Hospital-acquired urinary tract infection International journal of clinical practice, 57(5), 388–391.
[4] Pujades-Rodriguez et al. (2019): Lower Urinary Tract Infections: Management, Outcomes and Risk Factors for Antibiotic Re-prescription in Primary Care. EClinicalMedicine 14:23-31
[5] Gilboe, H. M., Reiakvam, O. M., Aasen, L., Tjade, T., Bjerner, J., Ranheim, T. E., & Gaustad, P. (2021): Rapid diagnosis and reduced workload for urinary tract infection using flowcytometry combined with direct antibiotic susceptibility testing. Plos one, 16(7), e0254064.
[6] Mott et al. (2020): A multinational European study of patient preferences for novel diagnostics to manage antimicrobial resistance. Applied Health Economics and Health Policy 18:69-79